
Written and medically reviewed by Dr. Ladan Eshkevari, CRNA, PhD, FAAN.
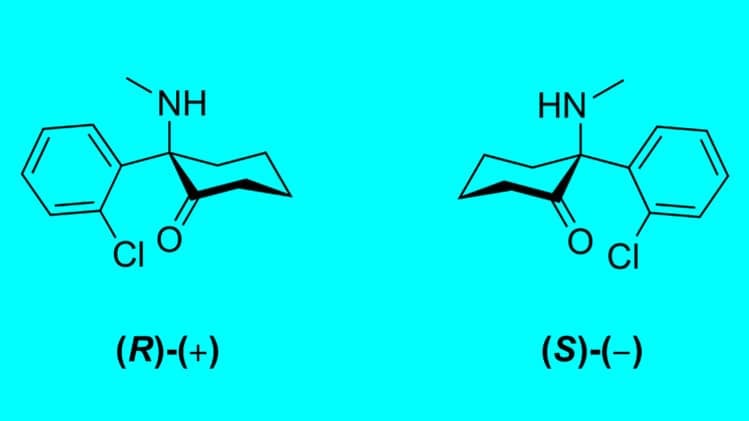
Ketamine exists in two mirror-image forms, S-ketamine and R-ketamine, and they differ in three ways that matter: potency, approval status, and how they are delivered. S-ketamine binds NMDA receptors about four times more tightly and is the form FDA-approved as Spravato (esketamine).[1][16] R-ketamine (arketamine) binds weakly, remains investigational, and is not available for treatment.[11]
Key takeaways
- Same molecule, two halves: S-ketamine and R-ketamine are enantiomers, not different medications, and clinical ketamine is usually a 50/50 racemic mix of both.[1]
- Only S-ketamine is approved: esketamine was approved as Spravato in 2019, and as of the current label it is indicated for treatment-resistant depression as monotherapy or with an oral antidepressant, and for depressive symptoms in adults with major depressive disorder with acute suicidal ideation or behavior.[13][16]
- R-ketamine is investigational: preclinical data suggest it may act longer with less dissociation, but the one larger human trial did not confirm an antidepressant advantage.[3][11]
- The experience differs: S-ketamine grips NMDA receptors far more tightly and is more dissociative, while R-ketamine binds weakly and feels more grounded in early research.[17][18]
- Route decides how much arrives: oral S-ketamine is only 8 to 11 percent bioavailable, which is why esketamine is a nasal spray and not a pill.[15]
What is the difference between S-ketamine and R-ketamine?
S-ketamine and R-ketamine are the two mirror-image halves of the same ketamine molecule. S-ketamine binds NMDA receptors about four times more tightly and is FDA-approved as Spravato. R-ketamine binds weakly, causes less dissociation, and is still investigational.[1]
Ketamine contains mirror-image molecules called enantiomers: S-ketamine (esketamine) and R-ketamine (arketamine). When you receive ketamine in a hospital for anesthesia or in a clinic for depression, you are typically receiving a 50/50 mixture of both, known as a racemic blend.
The two forms share the same chemical formula. Their different shapes determine how each one fits into receptors in your brain. Neither form is a “ketamine analog,” a separate compound built to imitate ketamine. They are the two halves of the ketamine molecule itself.
What is R-ketamine (arketamine)?
R-ketamine, also called arketamine, is the right-handed half of the ketamine molecule. It binds NMDA receptors weakly, produces little dissociation, and is currently investigational: available only through clinical trials, not as a prescribed treatment.[3][11]
Interest in arketamine comes from a specific hypothesis. Because it appears to activate growth factors such as BDNF more strongly while causing fewer dissociative effects, researchers have asked whether it could deliver ketamine’s antidepressant benefit without the sensory disruption.[2] That hypothesis is well supported in animal models and not yet confirmed in humans.[18]
Is S-ketamine stronger than R-ketamine?
Chemically yes, clinically it depends. S-ketamine binds NMDA receptors roughly four times more tightly, making it more potent per milligram and more dissociative.[1] Binding strength is not the same as clinical benefit, and dosing is adjusted for the difference.
The underlying numbers are specific. In receptor-binding work, S-ketamine’s inhibition constant at the NMDA receptor is 0.30 micromolar against 1.4 micromolar for R-ketamine, a difference of roughly four to five fold.[17] S-ketamine is likewise estimated to be about four times the anesthetic and analgesic potency of R-ketamine, and about twice that of the racemic mixture.[19]
Potency describes how tightly a molecule grips its target, not how well it treats depression. R-ketamine’s weaker grip is part of why researchers think it may cause fewer side effects, and early preclinical work suggests it may be better at driving the longer-term neuroplastic changes associated with durable remission.[2][3] That advantage has not held up in the larger human trial run so far.[11]
S-ketamine vs R-ketamine compared: potency, FDA status, route, and evidence
| Feature | S-Ketamine (Esketamine) | R-Ketamine (Arketamine) |
|---|---|---|
| Potency at NMDA receptor | High: inhibition constant 0.30 micromolar, roughly four to five times the affinity.[17] | Low: inhibition constant 1.4 micromolar.[17] |
| FDA status | Approved as Spravato nasal spray for treatment-resistant depression, as monotherapy or with an oral antidepressant, and for depressive symptoms in adults with MDD with acute suicidal ideation or behavior.[16] | Investigational, clinical trials only. Not approved.[11] |
| Administration route | Intranasal spray, in a certified clinic under observation for at least two hours.[16] | Intravenous in trial settings. No approved route.[9] |
| Evidence base | Large Phase 3 programs (TRANSFORM, SUSTAIN) plus multi-year real-world data.[4][5][6][12] | Animal models, one small open-label pilot, a case series, one Phase 2a trial.[3][9][10][11] |
| Primary brain effect | Rapid NMDA blockade producing a fast shift in glutamate signaling.[1] | Longer-term repair by stimulating growth factors such as BDNF.[2] |
| The dissociative experience | Moderate to high: perceptual shifts that peak near 40 minutes and generally resolve by about 90 minutes.[4] | Grounded: milder, with fewer dissociative effects in early research.[9] |
| Speed of relief | Significant symptom reduction seen by the second treatment in a 2025 real-world comparison.[8] | No clear advantage at 24 hours in the Phase 2a trial.[11] |
| Duration of relief | Effects can persist with continued dosing across a year of maintenance treatment.[6] | Animal studies suggest longer duration, unconfirmed in humans.[18] |
| Known limitations | Did not separate from placebo in adults 65 and older. Dizziness, dissociation, dysgeusia, vertigo, and nausea are the most common side effects, all monitored in real time during treatment.[7] | The Phase 2a trial (PCN-101) missed its primary endpoint at 24 hours.[11] |
How S-ketamine and R-ketamine affect the depressed brain differently
The two forms differ primarily in how tightly they bind NMDA receptors and potentially in how long their antidepressant effects last. Both trigger the release of glutamate, a chemical messenger that helps the brain regrow neural connections, but they take different biological pathways to do it.[1]
S-ketamine mechanisms
S-ketamine acts as a high-potency blocker of NMDA receptors, producing a rapid shift in glutamate signaling across brain regions. That high affinity drives both the immediate antidepressant signal and the dissociative out-of-body sensations.[17]
Some researchers theorize that S-ketamine’s effects may not last as long as R-ketamine’s, because it creates a temporary shift in brain signaling rather than supporting longer-term changes in how brain cells connect and function.
R-ketamine mechanisms
Arketamine has a much weaker grip on NMDA receptors, leading to almost no dissociative effect and a more grounded patient experience.
Preclinical research suggests R-ketamine may be superior at activating BDNF (brain-derived neurotrophic factor), a protein that acts like fertilizer for neurons. That points to a possible advantage in promoting the long-term structural changes needed to keep depression in remission.[2] This work is largely in animal models and has not been confirmed in large human trials.[18]
S-ketamine vs R-ketamine effects during treatment
The experience differs in intensity, clarity, and how detached or grounded patients feel. S-ketamine produces noticeable dissociation that peaks around 40 minutes and generally resolves by about 90 minutes. R-ketamine, in early research, produces a milder state without strong detachment.[4][9]
Esketamine effects
- creates a noticeable sense of dissociation, such as feeling separated from the body or surroundings
- can shift perception of time, space, and sensory input in a more noticeable way
- symptoms begin shortly after dosing, peak near 40 minutes, and generally resolve by about 90 minutes, attenuating with repeated dosing[4]
- the most common side effects, all monitored in real time during treatment, are dizziness, dissociation, dysgeusia, vertigo, and nausea[4]
- the label requires at least two hours of in-clinic observation after every dose, which is why we treat esketamine as an appointment rather than a prescription you take home[16]
Arketamine effects
- appears to produce a milder, more relaxed mental state in early research
- may involve subtle shifts in mood and perspective without strong detachment
- tends to feel less disruptive to awareness while still supporting antidepressant effects in early studies
- reported side effects are so far limited to mild blurred vision or dizziness without intense mental disruption[9]
Why the delivery route changes what reaches your brain
Route determines how much of a dose survives to reach the brain. Intravenous ketamine delivers essentially all of it. Intramuscular delivers about 93 percent. Intranasal delivers 45 to 50 percent. Oral ketamine delivers only 16 to 29 percent, because the liver breaks most of it down before it reaches circulation.[15]
The number that explains Spravato’s design is more specific. Taken by mouth, S-ketamine on its own is only 8 to 11 percent bioavailable, meaningfully worse than the racemic mixture, because S-ketamine undergoes greater first-pass metabolism in the liver.[15][19] A once-daily esketamine pill would waste roughly nine tenths of every dose. That is why the FDA-approved product is a nasal spray given under observation, not a tablet.
This is also why comparing the two enantiomers on potency alone is misleading. A form that binds four times more tightly but arrives at one tenth the concentration is not four times stronger in practice. When you read that one form is more potent, the practical question is always: potent by which route, at what dose, and how much of it actually got there.
For patients, the practical consequence is straightforward. IV ketamine gives clinicians precise control over dose and pace, which is why it remains the standard for infusion therapy. Spravato trades some of that control for a non-invasive route with an approved, insurance-recognized protocol. Neither is universally better, and the choice usually comes down to your diagnosis, your coverage, and how you respond.
What does the research say about S-ketamine for depression?
Esketamine became a prescription medication (Spravato) for depression in 2019 after large-scale clinical trials supported its safety and efficacy.[13]
Clinical trials supporting depression relief
Phase 3 efficacy and safety trials, such as the TRANSFORM program, showed that patients who added esketamine nasal spray to a new oral antidepressant saw a significantly greater reduction in symptoms than those using a placebo.[4] Those who continued treatment saw further improvement.
The relapse-prevention Phase 3 study (SUSTAIN-1) showed that patients who achieved stable remission on esketamine were about 51 percent less likely to relapse than those who switched to a placebo (hazard ratio 0.49).[5]
Long-term data from Phase 3 maintenance studies found that S-ketamine’s antidepressant effects can persist for at least one year of treatment, with no new safety signals and no evidence of lasting cognitive impairment.[6]
A 2026 real-world study extended these observations to an average of 2.5 years of esketamine treatment. In that single-clinic retrospective of 20 patients averaging 129 sessions each, 85 percent showed improvement in depression severity and 65 percent improved in anxiety severity.[12] Because the sample was small and had no control group, the findings are encouraging but preliminary.
Research limitations and open questions (S-ketamine)
Not every esketamine trial showed the same level of benefit across all patient groups. In the TRANSFORM-3 trial in adults aged 65 and older with treatment-resistant depression, esketamine plus a new oral antidepressant did not separate significantly from placebo at day 28 (p = 0.059).[7] Some patients still improved, and the effect was clearer in the 65 to 74 group than in those 75 and older, which suggests that age and overall health can influence how well treatment works.
A 2025 chart review of 153 patients found that IV ketamine produced a 49.2 percent reduction in self-reported depression scores by the eighth treatment, compared with 39.6 percent for intranasal esketamine. The IV group also improved faster, reaching a significant reduction after a single treatment rather than two.[8] It was a retrospective review at one health system, not a randomized comparison, so it describes what happened in practice rather than settling which treatment is better.
R-ketamine depression research

Arketamine research has grown as scientists look for ways to treat depression with fewer side effects.
Preclinical and early clinical findings
In animal models of depression, arketamine has shown stronger and longer-lasting antidepressant-like effects than S-ketamine, with fewer dissociative and behavioral side effects.[3][18]
Early human data is more limited but still informative. A small pilot study in patients with treatment-resistant depression found that a single intravenous dose of arketamine led to swift improvement in symptoms after one day, with minimal dissociation.[9] Additional case reports have followed patients after arketamine treatment and observed sustained improvements in mood and in social and vocational functioning.[10]
Research limitations and open questions (R-ketamine)
Despite strong early signals, larger R-ketamine trials have not yet confirmed an antidepressant advantage. In a Phase 2a trial of roughly 100 patients with treatment-resistant depression, the sponsor reported that arketamine (PCN-101) missed its primary endpoint: depression scores fell 15.3 points at 24 hours against 13.7 for placebo, a difference that did not reach significance.[11] Those results have not been published in a peer-reviewed journal as of July 2026. Most human studies on arketamine remain small, early-stage, or exploratory, with limited data on optimal dosing, treatment frequency, and long-term outcomes.
Why pharmaceutical companies developed esketamine first
Pharmaceutical companies focused on esketamine before racemic ketamine and R-ketamine because it offered a more practical path to regulatory approval. As a single enantiomer, S-ketamine could be packaged into a patented nasal spray with standardized dosing and tested in large, regulated trials.[14]
- S-ketamine could be developed as a proprietary single-molecule product rather than a generic racemic medication
- it fit a standardized nasal-spray model that worked well for large clinical trials
- it already showed enough antidepressant activity to justify major investment
- arketamine remained mostly a preclinical candidate while esketamine advanced through Phase 3 and Phase 4 studies
What this means for patients considering ketamine therapy
If you are considering ketamine therapy for depression, the difference between S-ketamine and R-ketamine comes down to what is available now.
- Esketamine (Spravato) is the established, regulated option, with insurance coverage for qualifying conditions.
- Racemic ketamine is commonly used in mental health clinics and contains both R and S forms working together. It is prescribed off-label for depression.
- R-ketamine on its own is not available outside clinical trials.
Choosing between them is less about which molecule is stronger and more about diagnosis, route, and coverage. For a treatment-by-treatment comparison including cost, see esketamine vs ketamine: difference, cost, and efficacy.
Frequently asked questions
What is the difference between S-ketamine and R-ketamine?
They are the two mirror-image halves of the same ketamine molecule. S-ketamine binds NMDA receptors about four times more tightly and is FDA-approved as Spravato. R-ketamine binds weakly, causes less dissociation, and remains investigational. Standard clinical ketamine is a 50/50 mixture of the two.[1]
Is S-ketamine stronger than R-ketamine?
Chemically yes. S-ketamine’s inhibition constant at the NMDA receptor is 0.30 micromolar against 1.4 micromolar for R-ketamine, so it is more potent per milligram and more dissociative.[17] Clinically, dosing is adjusted for that difference, so binding strength alone does not determine which works better.
Is R-ketamine available as a treatment now?
No. R-ketamine is investigational and accessible only through clinical trials. The options available today are FDA-approved esketamine (Spravato) and racemic IV ketamine, which is prescribed off-label for depression.[16]
Why is esketamine FDA-approved when arketamine is not?
Esketamine completed the large Phase 3 trials the FDA requires and was approved as Spravato in 2019.[13] Arketamine is still in early-stage research. Its one Phase 2a trial missed its primary endpoint, and those results have not been published in a peer-reviewed journal.[11]
Why is esketamine a nasal spray instead of a pill?
Because swallowing it wastes most of the dose. Oral S-ketamine is only 8 to 11 percent bioavailable due to first-pass liver metabolism, while the intranasal route delivers 45 to 50 percent.[15] The nasal spray is a pharmacokinetic necessity, not a preference.
Which is better for depression, S-ketamine or R-ketamine?
S-ketamine, on current evidence, because it is the only one with large controlled trials and FDA approval behind it. R-ketamine’s advantages are real in animal models but have not yet been confirmed in humans, and its one Phase 2a trial did not separate from placebo at 24 hours.[11][18]
Not sure whether esketamine or IV ketamine fits your diagnosis and your coverage? Request a consultation and we will walk you through both.
References
- Jelen LA, Young AH, Stone JM. “Ketamine: a tale of two enantiomers.” Journal of Psychopharmacology, 2021;35(2):109-123. PMID 33155503. pmc.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- Hashimoto K. “Molecular mechanisms of the rapid-acting and sustained antidepressant actions of (R)-ketamine.” Biochemical Pharmacology, 2020. PMID 32224141. pubmed.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- Hashimoto K. “Molecular mechanisms underlying the antidepressant actions of arketamine: beyond the NMDA receptor.” Molecular Psychiatry, 2021. nature.com. Accessed July 30, 2026.
- Popova V, Daly EJ, Trivedi M, et al. “Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant (TRANSFORM-2).” American Journal of Psychiatry, 2019;176(6):428-438. PMID 31109201. pubmed.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- Daly EJ, Trivedi MH, Janik A, et al. “Efficacy of Esketamine Nasal Spray Plus Oral Antidepressant Treatment for Relapse Prevention (SUSTAIN-1).” JAMA Psychiatry, 2019;76(9):893-903. PMID 31166571. pubmed.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- Wajs E, Aluisio L, Holder R, et al. “Esketamine Nasal Spray Plus Oral Antidepressant in Patients With Treatment-Resistant Depression: Assessment of Long-Term Safety in a Phase 3, Open-Label Study (SUSTAIN-2).” Journal of Clinical Psychiatry, 2020;81(3). PMID 32316080. pubmed.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- Ochs-Ross R, Daly EJ, Zhang Y, et al. “Efficacy and Safety of Esketamine Nasal Spray Plus an Oral Antidepressant in Elderly Patients With Treatment-Resistant Depression (TRANSFORM-3).” American Journal of Geriatric Psychiatry, 2020;28(2):121-141. PMID 31734084. pubmed.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- Meisner R, Li S, Boyle B, et al. “Comparative Effects of Repeated Ketamine Infusion Versus Intranasal Esketamine in Patients With Treatment-Resistant Depression: A Retrospective Chart Review.” Journal of Clinical Psychiatry, 2025;86(4):25m15789. psychiatrist.com. Accessed July 30, 2026.
- Leal GC, Bandeira ID, Correia-Melo FS, et al. “Intravenous arketamine for treatment-resistant depression: open-label pilot study.” European Archives of Psychiatry and Clinical Neuroscience, 2021;271(3):577-582. link.springer.com. Accessed July 30, 2026.
- Bandeira ID, et al. “Sustained antidepressant and functional response after arketamine in treatment-resistant depression: a case series.” 2024. sciencedirect.com. Accessed July 30, 2026.
- atai Life Sciences. “atai Life Sciences Announces Results From Phase 2a Trial of PCN-101 (R-ketamine) in Treatment-Resistant Depression.” Company announcement, January 6, 2023. Trial registry NCT05414422. ir.atai.com. Accessed July 30, 2026.
- Ayad N, Abdel Aziz K, Makhoul S, et al. “Long-term effectiveness and side-effects of intranasal esketamine in treatment-resistant depression: real-world, single-arm study of over 100 sessions.” BJPsych Open, 2026;12(1):e48. PMC12835693. pmc.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- U.S. Food and Drug Administration. “Drugs@FDA: NDA 211243, SPRAVATO (esketamine). Approval date March 5, 2019.” Accessed July 31, 2026.
- Jamed A, et al. “The development of esketamine versus racemic ketamine and arketamine: regulatory and pharmaceutical considerations.” Review, 2024. PMID 39428602. pubmed.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- Zanos P, Moaddel R, Morris PJ, et al. “Ketamine and Ketamine Metabolite Pharmacology: Insights into Therapeutic Mechanisms.” Pharmacological Reviews, 2018;70(3):621-660. Bioavailability by route: intramuscular 93 percent, intranasal 45 to 50 percent, oral racemic 16 to 29 percent, oral S-ketamine 8 to 11 percent. pmc.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- U.S. Food & Drug Administration. “SPRAVATO (esketamine) nasal spray, CIII: Highlights of Prescribing Information.” Revised January 2025. accessdata.fda.gov. Accessed July 30, 2026.
- Ebert B, Mikkelsen S, Thorkildsen C, Borgbjerg FM. “Norketamine, the main metabolite of ketamine, is a non-competitive NMDA receptor antagonist in the rat cortex and spinal cord.” European Journal of Pharmacology, 1997;333(1):99-104. Inhibition constants: (S)-ketamine 0.30 micromolar, (R)-ketamine 1.4 micromolar. sciencedirect.com. Accessed July 30, 2026.
- Yang C, Shirayama Y, Zhang J-c, et al. “R-ketamine: a rapid-onset and sustained antidepressant without psychotomimetic side effects.” Translational Psychiatry, 2015;5:e632. PMID 26327690. pmc.ncbi.nlm.nih.gov. Accessed July 30, 2026.
- Peltoniemi MA, Hagelberg NM, Olkkola KT, Saari TI. “Ketamine: A Review of Clinical Pharmacokinetics and Pharmacodynamics in Anesthesia and Pain Therapy.” Clinical Pharmacokinetics, 2016;55(9):1059-1077. PMID 27028535. pubmed.ncbi.nlm.nih.gov. Accessed July 30, 2026.

